
Oxfordshire’s maternity care

Many Clarion readers will have passed through the maternity ward of the John Radcliffe Hospital, whether as an infant or a parent. It is a place with which Oxfordshire, literally, has a familial bond.
But recently it hasn’t all been happy families. On Thursday, Baroness Amos published her Interim Report into maternity care across the UK, part of an ongoing investigation into failings of maternity care at hospitals across the country – including Oxford University Hospitals. Why is OUH under investigation, what does the report say, and what do parents say?
[Content warnings for this article: childbirth, stillbirth, neonatal intensive care, maternal health, racism, discrimination. We recognise this is a difficult subject for many readers.]
What is maternity care in Oxfordshire?
Oxfordshire has a comprehensive, and complex, maternity care service – largely under the auspices of Oxford University Hospitals (OUH). Despite the name, OUH includes hospitals across the county, including Banbury's Horton.
The expectant mother usually starts out with a GP appointment to confirm or register a pregnancy, and is then transferred to the community midwife team – or you can self-refer. This team is linked to a GP practice, but is run by OUH. The aim of the community midwife team is to co-ordinate care throughout pregnancy, and after the birth. The level of care needed through your pregnancy determines your pathway. An uncomplicated pregnancy means midwife-led care throughout, but at any point you can be transferred to consultant-led care.
For delivery there is a plethora of options. For straightforward pregnancies, you can choose to have your baby at home under midwife care, or at a midwife-led unit like Wallingford Birthing Centre or the Horton Hospital in Banbury. Birthing pools, mood lighting, 24 hour care and maternity support workers are on hand to support with the first few hours and those first feeds. There is a midwife led unit in the John Radcliffe, too, called the Spires.
But if your pregnancy or delivery at any point becomes complicated, you will be transferred to consultant-led care, which means a trip to the JR. (Banbury's Horton Hospital formerly had consultant-led care: it has been the subject of a long running campaign, firstly to prevent its downgrading to midwifery-led care, and latterly a Bring Back Births to Banbury campaign to return the Horton to full obstetric care.)
The JR has the full set: a midwife-led unit, a delivery suite, and for high-risk cases the Silver Star. It receives referrals from across the Thames Valley, and consequently is impressively equipped with a special care baby unit, a Neonatal Intensive Care and High Dependency Unit, a Children's Hospital, a Ronald McDonald House and other facilities such as an Infant Feeding Team and a Human Milk Bank.
Why the noise?
On paper, few hospitals are better equipped. Yet in recent years, maternity care at the JR has been dogged by controversy.
An active campaign group, ‘Families Failed by Oxford University Hospitals’, has been highlighting their experiences since 2024, with some 750 families campaigning to make their voices heard. Banbury MP Sean Woodcock said that one of the first things he did after taking office was “stick the dossier of maternity failings compiled by local Horton Hospital campaigners on Health Secretary Wes Streeting's desk”. This dossier later appeared in a BBC report, ‘Campaigners tell harrowing birth stories’.

What does the data say?
Maternity data is compiled and published by MBRRACE (Mothers and Babies; Reducing Risk Through Audits and Confidential Enquiries), a national collaboration run by the University of Leicester and the University of Oxford.
In 2023, the latest year for which data is available, OUH had the worst stillbirth rate in the UK. Its stillbirth rate has been graded red (at least 5% higher than the average for comparable trusts) or amber (higher than the average rate but within 5%) ever since these figures began to be analysed in 2017.
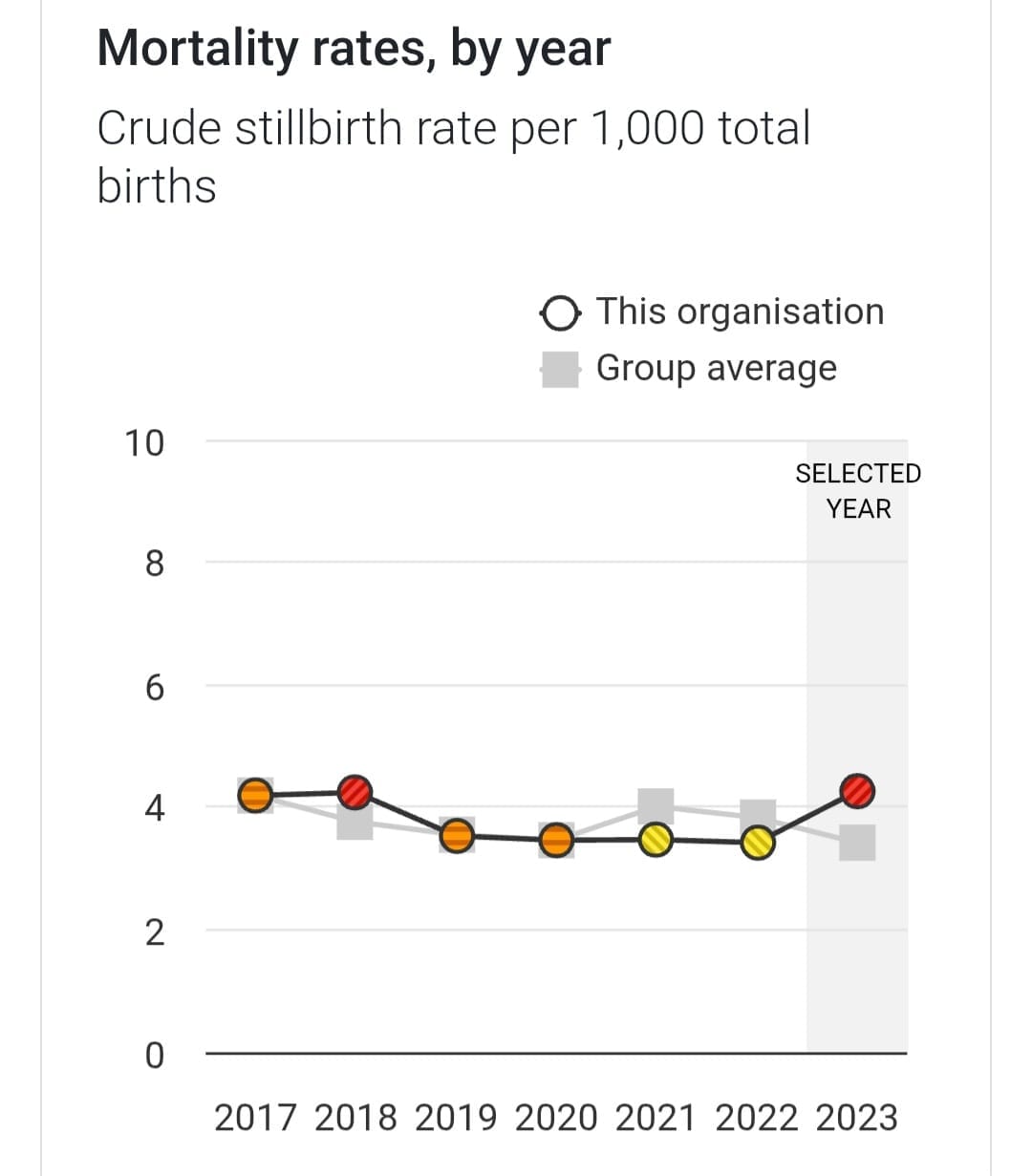
The rest of the data puts Oxford squarely mid-table in terms of mortality rates for NICU (neonatal intensive care unit) and neonatal surgery.
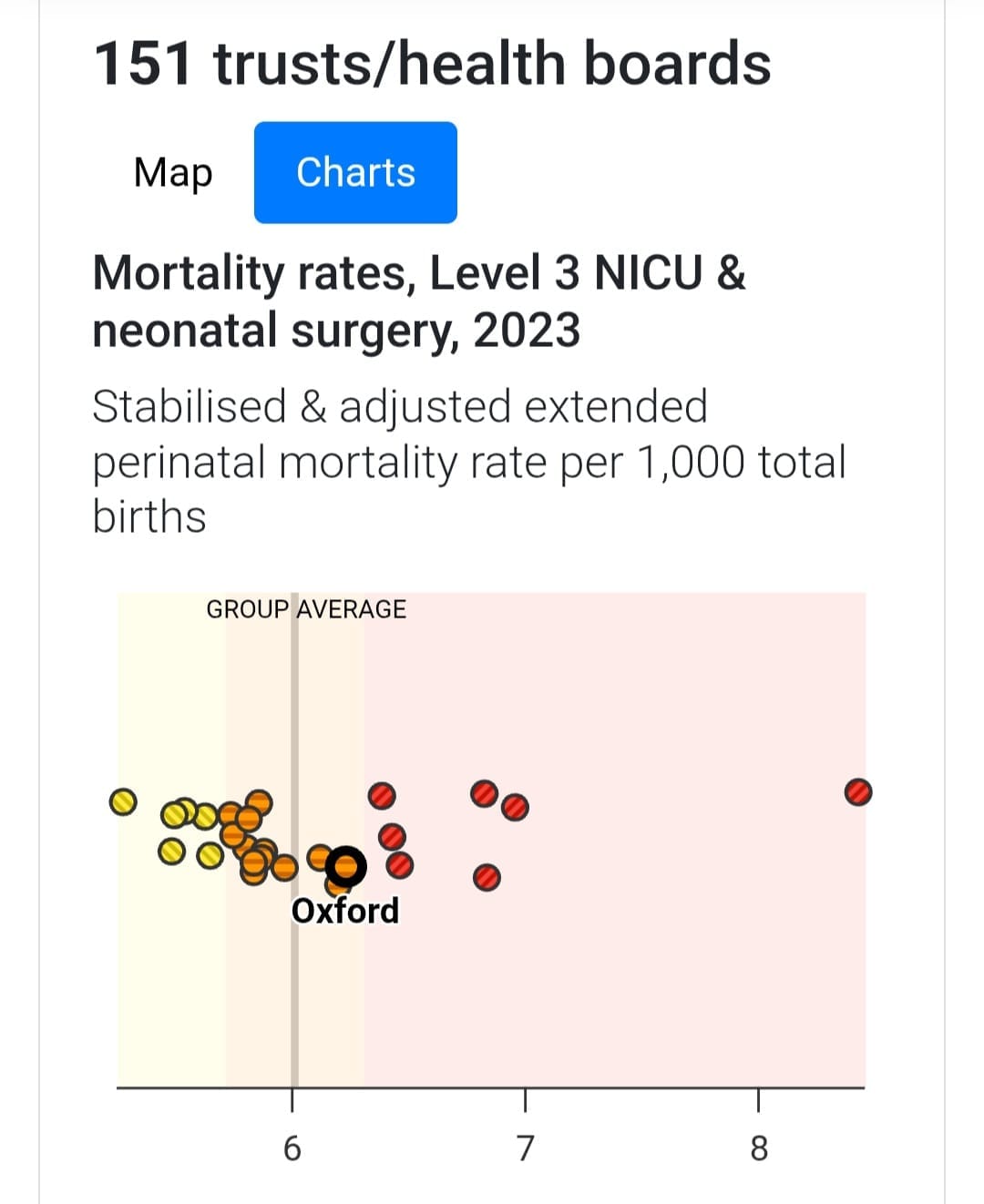
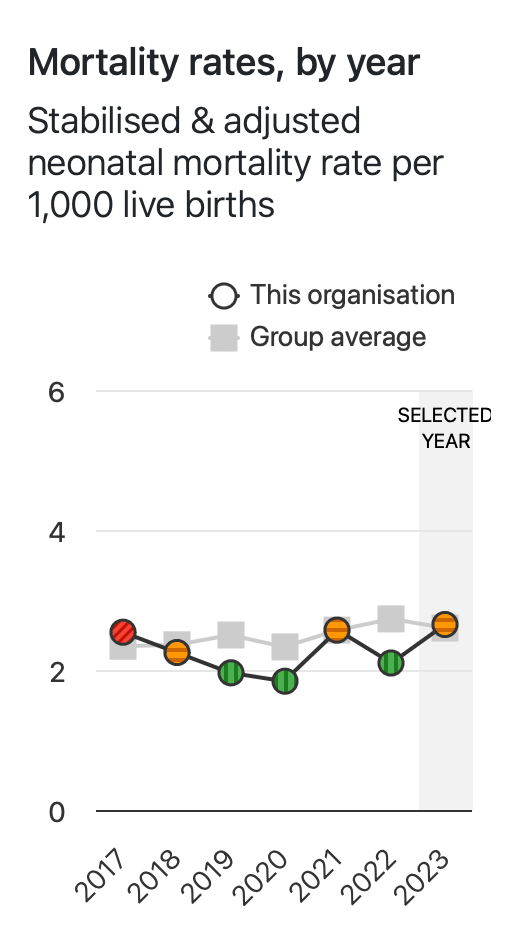
MBRRACE © 2025 University of Leicester and University of Oxford
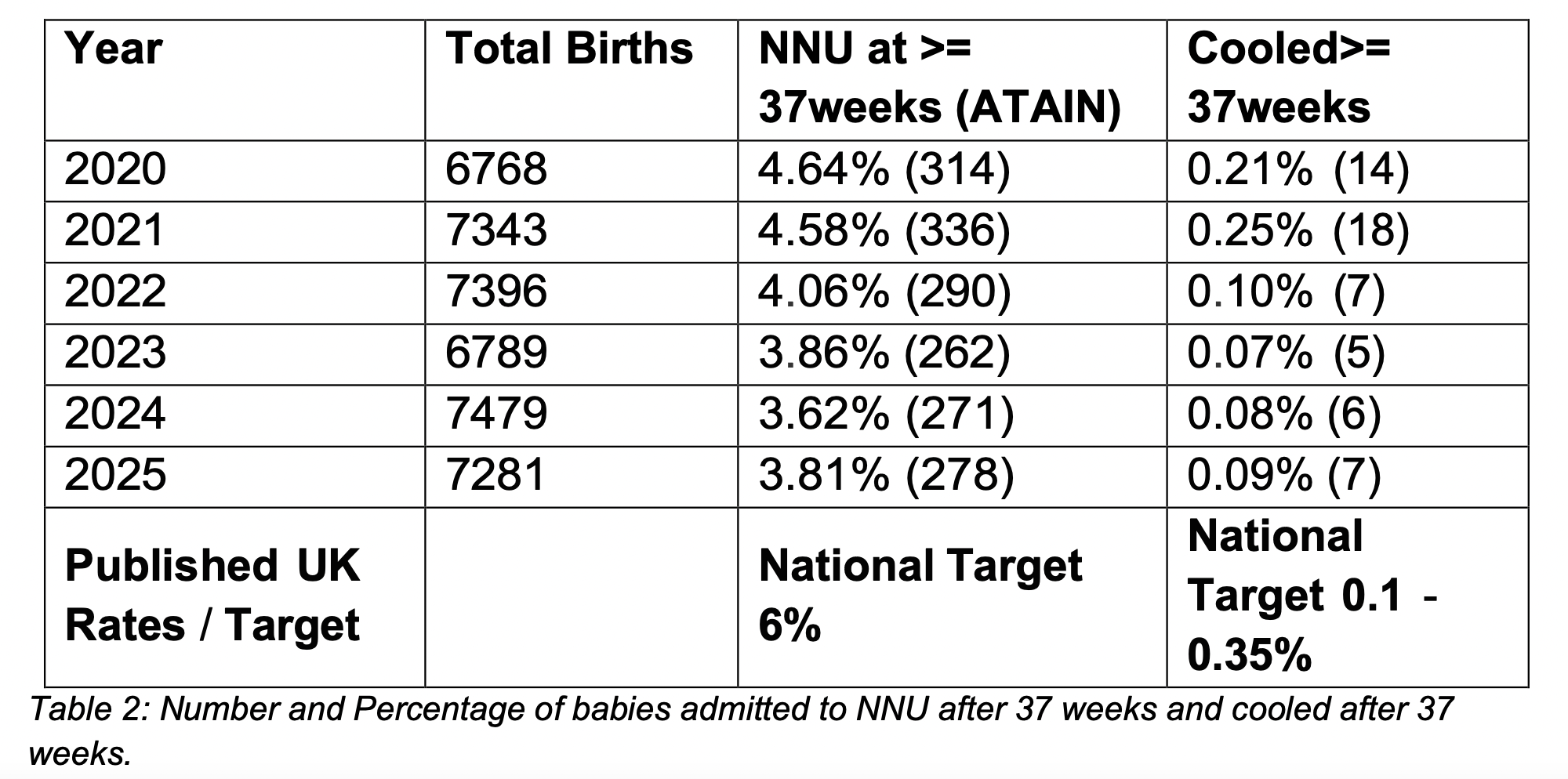
Moving onto statistics compiled by OUH themselves, the Trust monitors two key indicators for birth injuries in babies: full-term admissions to neonatal units, and the number of babies requiring therapeutic cooling due to low oxygen levels at birth. Over time, OUH has improved on both measures such that it is well below the national target.
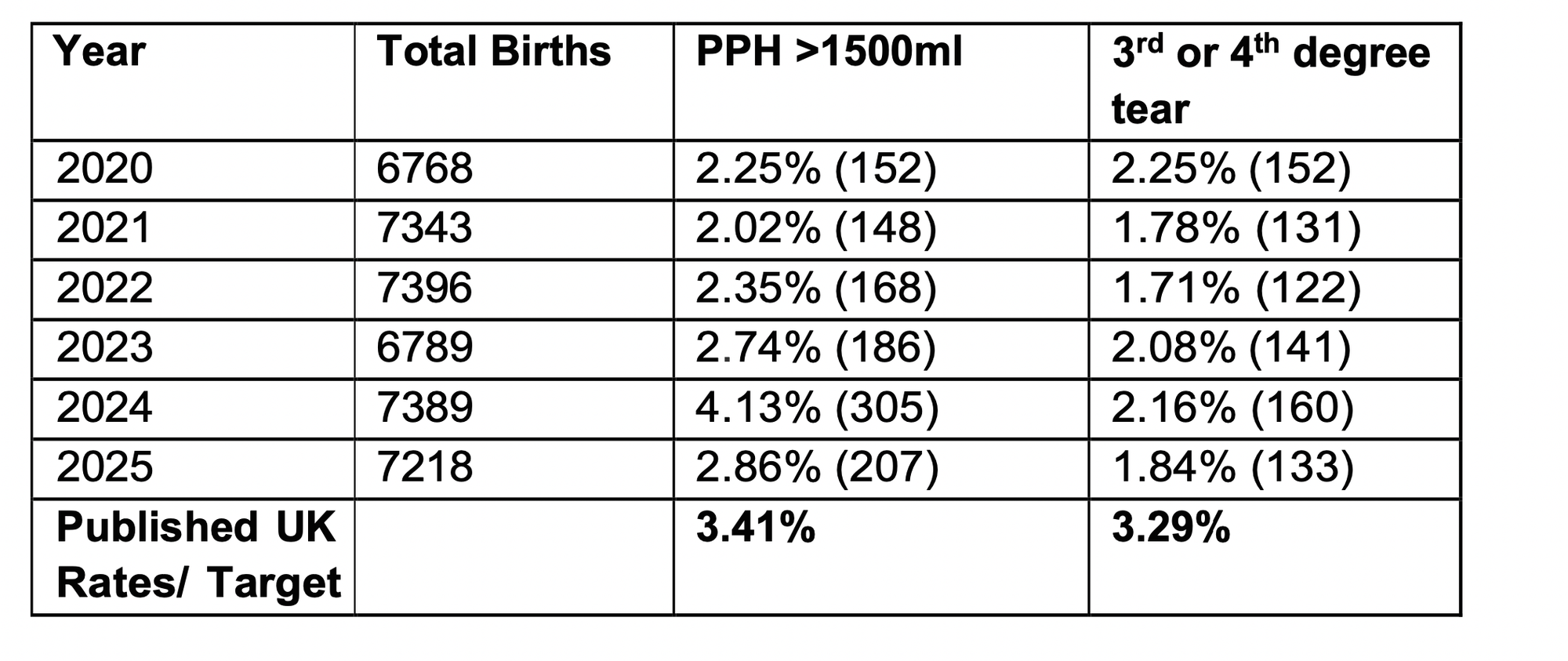
If we look at maternal health, the Trust benchmarks postpartum haemorrhage (PPH) >1500ml and third- or fourth-degree perineal tears and benchmarks performance against national standards. Here the trust remained, since 2020, consistently above UK target rates.
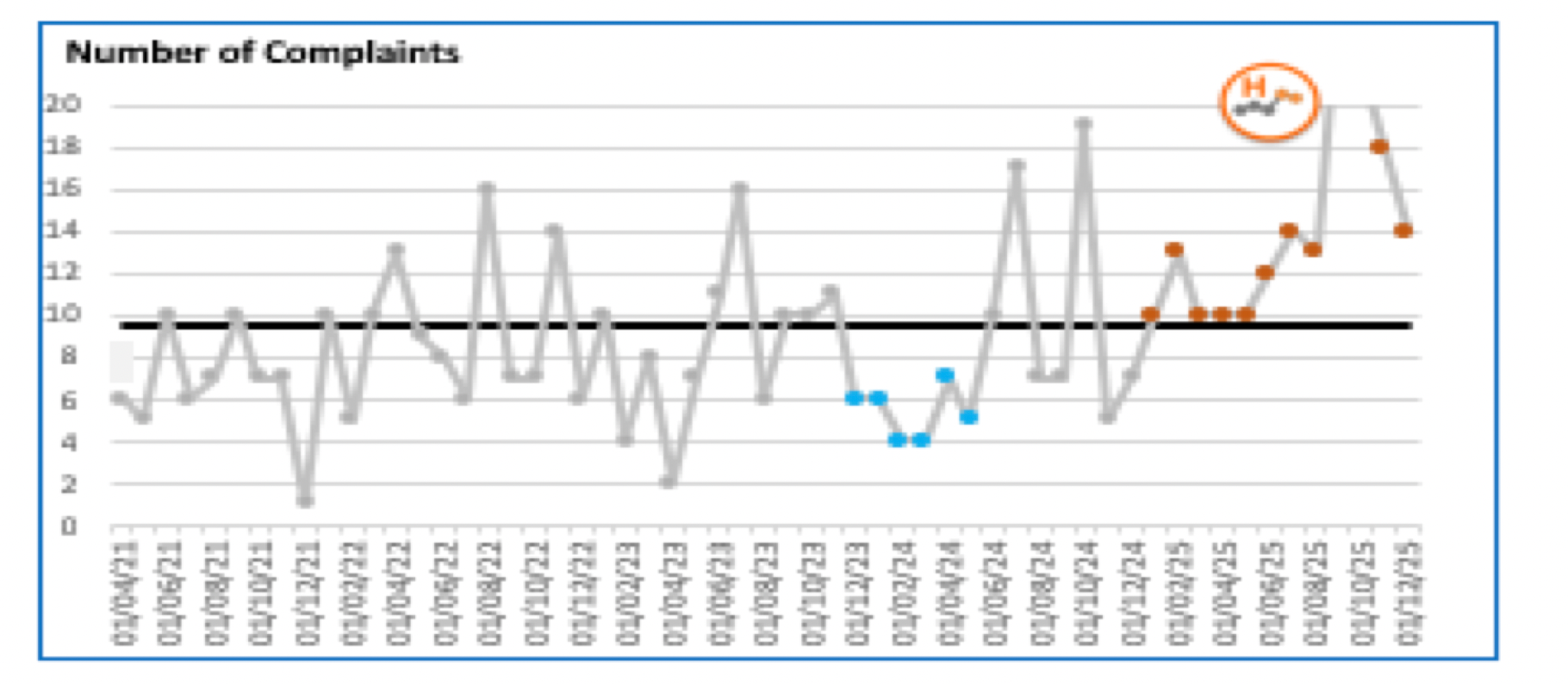
Complaints, however, have risen sharply since September 2025 – with a “significant proportion relating to care delivered in previous years”. The most common themes are communication, consent, and postnatal care, according to a report presented to Oxfordshire County Council’s scrutiny committee on 29 January.
National headlines
In 2021, the Care Quality Commission (CQC) had carried out an unannounced focused inspection of the main maternity department in the John Radcliffe hospital. It also visited the Cotswold Birth Centre (Chipping Norton) and the Horton Midwifery-Led Unit in May after receiving “information of concern” about the culture of the department. As a result of its inspection, it downgraded the rating for maternity services from “good” to “requires improvement”, writing:
“Although most staff said they were encouraged to be open and honest with people when things went wrong, some staff reported that they were not always comfortable raising concerns without fear of what would happen if they did. Some said they felt that communication between senior management and staff was not always effective.”
At the Cotswold Birth Centre, in particular, this had uncanny echoes of an episode in 2012 when two midwives were suspended amid allegations of bullying – leading to the short-term closure of the unit. Campaign group Families Failed by OUH Maternity Services (FFOMS) believes there is a long-standing culture issue.
“These are not the consequences of understaffing or finances. They are the consequences of a toxic institutional culture with practices consistent with deep-rooted paternalism and, we believe, institutional misogyny. What makes OUH uniquely deserving of a public inquiry is not only the extent of the harm, but that it has been allowed to happen. Oversight mechanisms have demonstrably failed to identify and address the pattern of harm we have documented. When families harmed by OUH speak out they are silenced, dismissed, and even blamed. Families tell us that medical records go missing or are altered. Confidential, sensitive information is released by data breaches. Complaints processes are plagued by reputation management tactics.”
Until November 2025, this disquiet had been little noticed outside Oxfordshire. But that month, a four-month investigation by the New Statesman and Channel 4 News hit the headlines. It led with the claim of the stillbirth rate, but also featured stories from 24 women whose care ranged from 2009 to 2025. (Around 7,000 women give birth in OUH each year.)
The article cites “accounts of stillbirths and neonatal deaths; mothers whose children have been left with brain damage and who have themselves sustained lifelong injuries and mental trauma”. FFOMS has equally harrowing stories:
“A full-term baby died in 2015 after repeated maternal requests to deliver the baby were ignored. A mother was not anaesthetised for her emergency caesarean in 2003, shouting at the surgeon to stop, her screams loud enough to be heard from the corridor. Until 2021, OUH implemented a policy that contravened NICE guidelines and, in our view, was inconsistent with the Montgomery ruling on informed consent.”
This is a reference to OUH’s former practice of refusing mothers’ requests for Caesarean sections unless clear medical need was demonstrated. The New Statesman article spotlights another departure from standard practice, the insistence on a 36-week scan for all mothers; campaigners believe this has resulted in scans being denied at other stages of pregnancy, even in high-risk situations.
While the ratings have not been amended since 2021, the CQC published results from their 2024 and 2025 annual maternity surveys. These found that feedback from users of OUH maternity services (sample size of 256) was “about the same” as other trusts in 55 out of 58 questions – but care in hospital after the birth was “somewhat worse than expected”. OUH has since launched a Perinatal Improvement Programme, focusing on Service User Experience, Safety, and Staff Experience.
The Amos investigation
In June 2025, Health Secretary Wes Streeting launched a rapid national investigation into NHS maternity and neonatal services. Baroness Amos (coincidentally also Master of University College), was appointed to lead this investigation to examine “the systemic causes of unacceptable care affecting women, babies, and families”.
12 trusts are being investigated by Baroness Amos, of which OUH is one. The Government has not published the criteria for inclusion, but Baroness Amos noted:
“When selecting Trusts for the local investigation phase, I wanted to make sure that there was sufficient variety, not just geographically but also in terms of demographics, the mix of cases and the different types of Trust. In selecting Trusts, I also took into consideration poor outcomes, such as perinatal mortality rates, and poor experience, such as patient survey data, in addition to Trusts proposed by bereaved and harmed families who had experienced failures in maternity care.”
Within its first six months, she visited all 12 trusts, including OUH. FFOMS attended four formal evidence-gathering sessions with her in October.
In December, she set out her ‘Reflections and Initial Impressions’. They set out a likely need for “systemic change” across maternity care in England, with consistent issues across trusts including:
- a lack of communication and support from clinical teams and organisations;
- women not being listened to or given the right information to make informed choices at critical moments of their care, as risk profiles change;
- women’s knowledge of their own bodies, such as reduced fetal movement, sometimes being disregarded;
- fathers and non-birthing partners feeling unsupported;
- the impact of discrimination against women of colour, working class women, women with mental health challenges and younger parents leading to poorer outcomes;
- a lack of empathy, care or apology, with women feeling blamed and guilty, and a lack of recognition of substandard care;
- an overly legalistic, adversarial approach when concerns or complaints are raised;
- the failure of regulatory bodies to protect vulnerable women and families, and the perception of health professionals and organisations ‘marking their own homework’;
- poor standards of basic care, such as lack of cleanliness;
- women and families finding it difficult to access their medical notes (and notes being redacted or observations filled in at a later date);
- women and families being placed in inappropriate spaces after loss or harm (for example, being put on wards with newborns after they have experienced a loss).
Then, in January, the next stage of the inquiry saw a call for evidence (open until 17 March). Two surveys are available: one for women to share their experiences of maternity and neonatal services, and one for others to share their experiences supporting someone through pregnancy.

Interim report
Which brings us to the current Interim Report. The report is careful not to name any specific trusts. Instead, it concentrates on systemic failings or challenges that appear to be common across multiple trusts; understanding why negligent, poor, good and excellent practice can coexist; the drivers of consistent, sustained and safe care; and how these can be replicated.
So far, we learn that Baroness Amos believes there to be the following challenges across the NHS, with select quotes from the interim report.
- A challenging culture within some NHS trusts, organisationally, in teamwork, and in from leadership. Staff described instances where conduct fell markedly short of social and workplace norms, including verbal aggression. (“Please, can you tell them we need help to put pride back into our profession?” – Midwife)
- Discrimination, notably among women of colour, women living in more deprived areas, and LGBTQ+ families. During a stakeholder panel, a community organisation reported a hospital staff member who trained students saying “the bloody Asian ones just go on and on and on”. LGBTQ+ families reported that services focus narrowly on “mothers” and “fathers” and fail to reflect diverse family structures. One family member said “I almost died in birth, as I had my baby – I was then asked questions like ‘who was the real mum?’”
- Poor responses and a lack of accountability when things go wrong, including a lack of compassion, and transparency in the aftermath of incidents that had resulted in harm, including birth trauma and baby loss. This included ambiguity regarding whether their baby had been born alive.
- Ageing hospital buildings, including leaking roofs, fire hazards, rooms that were not big enough to accommodate equipment, and bereaved mothers having to receive care in a ward shared with women in active labour. “When we moved rooms, I said — because [name] was on me at this point, and I remember saying, ‘I don’t want to scare anyone else’, because I knew that they were going to wheel me through delivery suite, and I remember saying to them, ‘I don’t want other mums seeing us, like, I don’t want to scare them’. And a midwife said, ‘Nobody will know, nobody will look at you and know. You just hold her.’ […] I had to go through delivery suite, and I could hear mums in labour, it’s all I could hear”. (Family member)
- Workforce: Staff said that, despite their desire to give quality care to patients, high turnover of staff and a reliance on midwives (who do not provide frontline care) meant they could not perform at their best. Increasing complexity of maternity and neonatal services also creates a highly pressurised work environment. One family described not having access to bereavement support for days after their baby died, “so we lost on the Friday and it wasn’t until Monday that we had any specific bereavement care because the bereavement midwives just work office hours”. (Family member)
Not everything can be laid at the feet of the NHS or individual trusts. There are wider social issues here, as well as an organisation, and its consultants, still adjusting to the age of deference being replaced by the age of social media. Misinformation and lack of nuance are everywhere. The investigation continues, and the call for evidence remains live.
Early reactions

Simon Crowther, interim Chief Executive Officer at Oxford University Hospitals, said:
“We would like to thank the families and staff members who have spoken honestly and openly to Baroness Amos and her team. We know it will have taken great strength for those sharing difficult experiences and we are very grateful to them for doing so. It is already helping us to make improvements and to identify areas of good practice we can build upon. We very much welcome the national investigation.”
As well as being Oxford West & Abingdon MP, Layla Moran is Chair of the Health & Social Care Select Committee. She was unequivocal:
“It is heartbreaking to yet again hear the stories of families failed tragically by the system, but also of healthcare professionals who have faced vitriol for doing their jobs in difficult circumstances. The committee's message is clear: don’t wait to start making changes. The excuses for any more delay have run out.”
Freddie van Mierlo, MP for Henley & Thame, added:
“That services are failing too many women, babies, families and staff is a devastating conclusion. At the same time, it is important to recognise the hundreds of hardworking NHS professionals at Oxford University Hospitals and across the country who continue to provide compassionate and essential care in extremely challenging circumstances. Many staff are working under intense pressure. Too often, defensive and inadequate responses have compounded trauma and undermined trust; there needs to be a complete culture shift in listening to and responding to harmed families.”
Families Failed by OUH Maternity Services says that the interim report misses the elephant in the room.
“The findings confirm what bereaved and harmed families have documented for years: women’s concerns dismissed, notes amended or redacted, babies registered as stillborn in circumstances that demanded independent investigation, and complaint processes that prioritise institutions over harmed families. What is notably absent in the interim report is any reckoning with the ideology that has driven preventable harm – the institutional promotion of “normal birth” that prioritised a “watch and wait” approach and treated intervention as failure. That thread runs through this report’s own data, but it is not named.”
What more can we expect?
The Amos inquiry is unlikely to make recommendations for Oxford University Hospitals specifically. Its aim is “one set of national recommendations”. OUH, and the other 11 trusts, are the supporting evidence.
But it was OUH, not the others, that hit the headlines in November. It was OUH, not the others, that consistently had the highest stillbirth rate. It is unescapable that Baroness Amos’s recommendations will be strongly informed by what she has found at OUH, and that the trust will be expected to implement these recommendations post haste. But FFOMS says only a separate inquiry into OUH will provide the answers they seek.
“No national investigation, however thorough, can examine these specifics with the depth they require. Only a dedicated public inquiry, with full powers of disclosure, can establish what OUH knew, when it knew it, and what it chose to do. Only a public inquiry can establish why this horrific harm was not only allowed to continue but actively managed to protect institutional reputation.”
We should never doubt that the small groups of committed campaigners can make a difference. Families Failed by OUH and Keep the Horton General have catapulted maternity services at OUH up the list of trusts for investigation, perhaps precipitating change on a national scale.
Giving birth is a deeply personal and powerful experience, whether it is the dream birth envisaged in the lead-up, frequent trips to the Women's Centre throughout pregnancy, or a confusing medical scramble at the end. The results of the inquiry matter both to those who feel they have suffered in recent years, and to many Oxfordshire mothers and children to come.
Sources and further reading
- Baroness Amos' 'Reflections and Initial Impressions' on her investigation into Maternity and Neonatal Services in England
- Baroness Amos' Interim Report published 26 February 2026
- Original Channel 4 and New Statesman coverage (£)
- Further New Statesman coverage in the aftermath of the original accusations (£)
- Care Quality Commission's 2025 Maternity Survey (national)
- OUH response to Care Quality Commission 2025 Survey Results
- Health Secretary Wes Streeting's statement to the Commons sharing a progress update on the Amos report
- Royal College of Midwives response to Baroness Amos' interim report
- Families Failed by OUH Maternity Services
Support
We recognise that this article may have been as hard to read as it was to write. Here are some sources of support, should you need them.